Momentum is building to end medical co-pays in prisons and jails
Three states have taken action in 2019 to change one of the most harmful policies in prison healthcare.
by Wanda Bertram, August 8, 2019
Prison healthcare is almost always a depressing topic, but not today, when we can report an important victory: Illinois recently became the third state in 2019 to reform the practice of charging medical co-pays to incarcerated people.
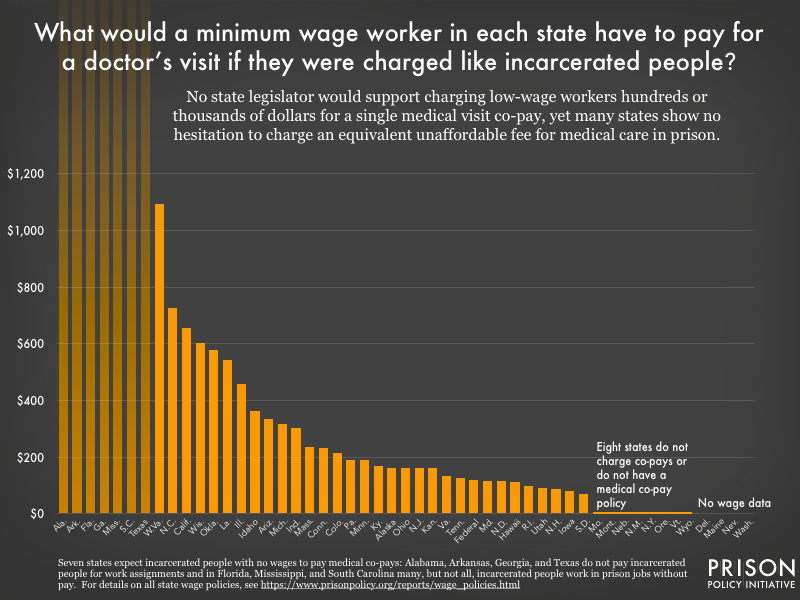
Previously, we published a state-by-state analysis showing that most prisons charge medical copays to people inside – despite the fact that their patients are impoverished and earn little to no money for their work in prisons. Using prison and free-world wage data, we calculated what each state’s co-pay would cost if it was charged to free-world patients making the minimum wage. Our analysis revealed that fourteen states charge co-pay amounts equivalent to charging minimum wage workers over $200.
 Policy details and sourcing information can be found in the Appendix of our original analysis.
Policy details and sourcing information can be found in the Appendix of our original analysis.
Charging co-pays to incarcerated people to shore up a state’s correctional budget is simply wrong. In our analysis, we explained that not only does this policy squeeze poor people and their families; it hurts public health by making the choice to seek medical attention a costly one.
We’re glad to see that states are now paying attention and taking action:
- Illinois Governor J.B. Pritzker signed a bill in July eliminating the state’s $5 co-pay. Previously, people working in an Illinois state prison (where the minimum wage is 9 cents per hour) would have had to work for over 55 hours to afford the $5 fee. That’s like charging a non-incarcerated minimum-wage earner in Illinois over $460. In some cases, incarcerated people paid even more before getting adequate care, because paying the fee didn’t guarantee a doctor visit – only that a nurse would review one’s medical request.
- Earlier this year, the California Department of Corrections and Rehabilitation announced that it would stop charging a $5 medical co-pay to incarcerated people. CDCR’s press release acknowledged what advocates have long known: Charging co-pays is bad for public health. “Copayments,” it said, “may hinder patients from seeking care for issues which, without early detection and intervention, may become exacerbated.” The department’s decision came as the California legislature was considering AB 45, a bill to eliminate medical co-pays in both state prisons and county jails. AB 45 (for which we wrote a letter of support) continues to move through the state legislature.
- The Texas legislature stopped short of eliminating medical co-pays in prisons entirely, but made progress by replacing the notorious $100 fee Texas had charged incarcerated people with a $13.55 per-visit fee. While this change marks a substantial improvement, incarcerated people in Texas – who earn nothing for their labor – will continue to be charged the highest medical co-pay in state prisons nationwide.
State reforms like these can’t come soon enough. As we noted in our 2017 analysis, out-of-reach co-pays in prisons and jails have two inevitable and dangerous consequences. First, when sick people avoid the doctor, disease is more likely to spread to others in the facility – and into the community, when people are released before being treated. Second, illnesses are likely to worsen as long as people avoid the doctor, which means more aggressive (and expensive) treatment when they can no longer go without it.
It’s welcome news that states are finally taking action to change this risky and regressive policy. Will your state be next?



